
Keratoconus & Corneal Crosslinking
(圆锥角膜与治疗)
What is keratoconus?
Keratoconus is an eye condition that causes the cornea to become progressively thin and bulge into a cone shape (i.e. corneal ectasia). It is the most common cause of corneal ectasia worldwide. The irregular corneal shape affects how light enters the eye, leading to blurred vision, glare, and increased sensitivity to light.

Photo credit: David Yorston. Community Eye Health 2009;22:71.
Symptoms of keratoconus
- Blurred or distorted vision
- Double vision
- Increased sensitivity to light and glare
- Frequent changes in glasses prescription
- Difficulty seeing at night
If left untreated, keratoconus can significantly affect daily activities, making it harder to drive, read, or recognise faces.
Causes & Risk Factors
Eye rubbing has been shown to be the single most important risk factor for keratoconus. Other risk factors may include:
- Genetic predisposition and positive family history of keratoconus
- Allergic eye disease (which is linked to eye rubbing)
- Underlying medical conditions (e.g. Down syndrome, Marfan syndrome, Ehler-Danlos syndrome)
- Hormonal influence (keratoconus may worsen during puberty or pregnancy)
Treatment
The treatment of keratoconus depends on the severity and progressiveness of the disease. Early detection and management is vital to preserve the vision. We will perform a comprehensive eye examination and discuss with you the best possible treatment plans.
1. Early / conservative management
- Lifestyle management: Avoid eye rubbing, treatment of allergic eye disease
- Spectacles
- Contact lenses (CL) - soft CL, rigid gas permeable (RGP) CL, hybrid CL, piggyback CL, scleral CL
2. Surgical management
- Corneal crosslinking (CXL): A minimally invasive procedure that strengthens the cornea and halts disease progression. It is most effective in early to moderate stages. This treatment aims to stabilise the disease but not to improve the vision (though some studies showed ~10% improvement in vision after CXL). This is the only treatment that addresses the root cause of keratoconus (i.e. weakening of the cornea).
- Intracorneal ring segments (ICRS): Small ring segments, either synthetic or donor human corneal tissues (CAIRS), can be implanted to improve the shape and curvature of the cornea in keratoconus.
- Corneal transplantation: This may be in the form of deep anterior lamellar keratoplasty (DALK) or penetrating keratoplasty (PKP). DALK is preferred when the corneal endothelium is not affected.
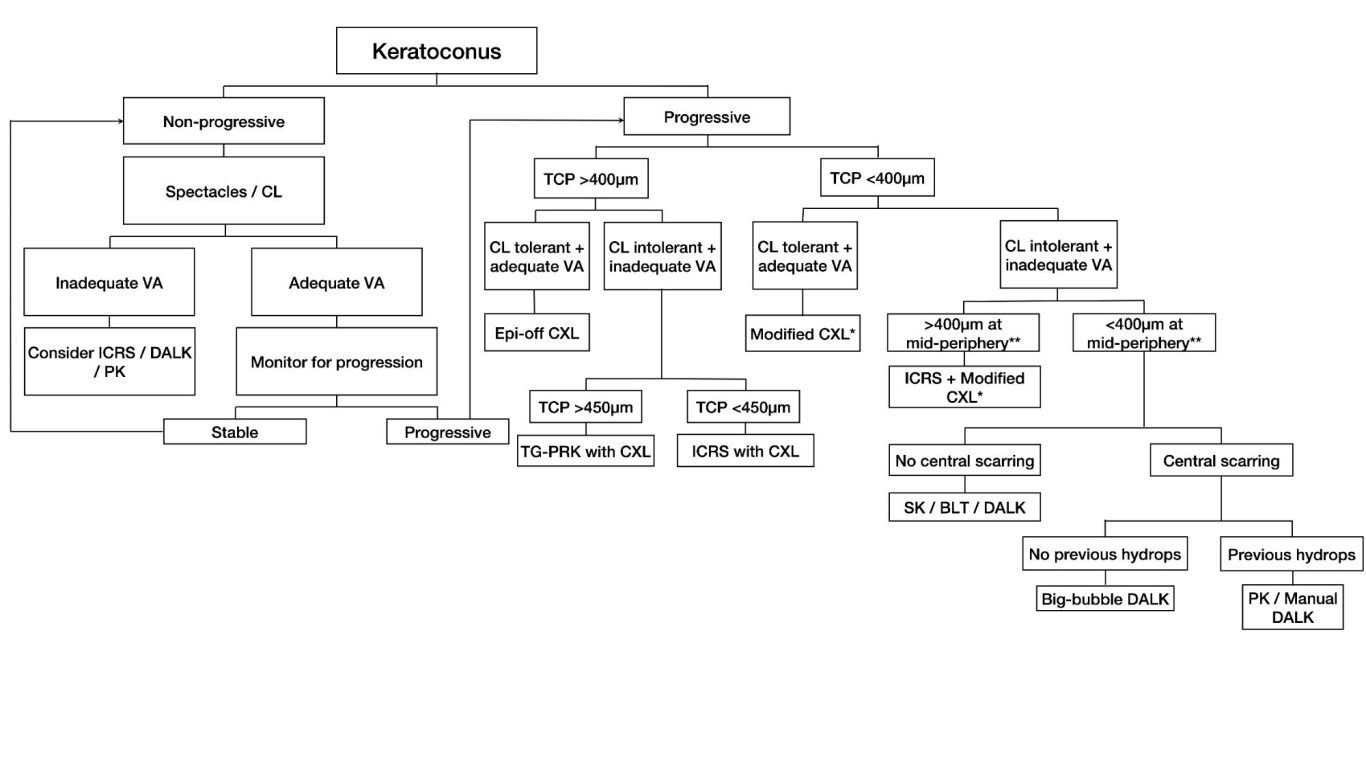
A proposed treatment algorithm for guiding the management of keratoconus. CL, contact lens; VA, visual acuity; ICRS, intracorneal ring segments; DALK, deep anterior lamellar keratoplasty; PK, penetrating keratoplasty; TCP, thinnest corneal pachymetry; CXL, corneal cross-linking; TG-PRK, topographic guided-photorefractive keratectomy; SK, stromal keratophakia; BLT, Bowman’s layer transplantation; DM, Descemet membrane. *Modified CXL includes transepithelial, iontophoresis-assisted, lenticule-assisted, CL-assisted, and adapted fluence CXL. **Corneal thickness at the mid-periphery/tunneling site for ICRS implantation. This figure is reproduced from the published article: Deshmukh R, Ong ZZ, Rampat R, Alio de Barrio J, Barua A, Ang M, Mehta JS, Said DG, Dua HS, Ambrosio R Jr, Ting DSJ. Management of keratoconus: An updated review. Front Med 2023;10:1212314.
What is corneal crosslinking (CXL)?
Corneal crosslinking (CXL) is a minimally invasive procedure designed to strengthen the cornea and halt the progression of keratoconus and other corneal ectasias.
How does CXL work?
The procedure is usually performed as a day case under local anaesthesia (with eye drops only), and the surgery takes around 20-30 minutes to complete. General anaesthesia may be used in some cases when needed. CXL involves the use of riboflavin (vitamin B2) drops and ultraviolet A (UVA) light irradiation to achieve crosslinking and strengthening of the cornea.
Types of CXL
- Epithelium-off (standard CXL): The outer layer of the cornea (epithelium) is removed to allow better absorption of riboflavin.
- Epithelium-on (transepithelial CXL): The epithelium is left intact, offering faster recovery with slightly reduced effectiveness.
- Accelerated CXL: Uses a higher UV intensity over a shorter duration for quicker treatment, usually around 10 minutes (as opposed to 30 mins for the conventional Dresden protocol)
N.B. Mr. Ting's preferred approach is the epithelium-off, accelerated CXL method. In cases with thin cornea, contact lens-assisted CXL method is used.
The procedure
- Anaesthesia: The procedure is usually performed under local anaesthetic, meaning you remain awake but feel no pain. However, general anaesthesia may be required occasionally due to patient preference or certain underlying conditions.
- Start of procedure: A sterile drape will be placed over the face. Then, a lid speculum will be inserted to help hold the eye open.
- Removal of corneal epithelium: The central 8-9 mm of corneal epithelium will be removed, either with alcohol-assisted approach or manual removal with a blunt surgical blade. This is to ensure a better penetration of the riboflavin drops into the cornea.
- Administration of riboflavin drops: Riboflavin drops will be applied onto the cornea every 1-2 minutes for 10 minutes.
- UVA irradiation: UVA light is directed to the cornea for 10 minutes (accelerated protocol) to achieve the crosslinking effect.
- Aftercare: A bandage contact lens is placed onto the cornea to ensure comfort and will be removed 5-7 days later. A course of topical antibiotics, steroids and anaesthetic eye drops and/or pain relief tablets will be given. The patient may experience some eye discomfort or pain during the first 1-3 days, and usually recovers within 3-7 days.
Potential risks
CXL is a minimally invasive procedure with good safety profile. However, like any medical procedure, it carries some potential risks. These may include:
- Corneal infection (<1% chance), usually during the first 1-3 days when the corneal epithelium has not fully healed.
- Corneal haze (uncommon), usually responds to topical steroids eye drops.
- Corneal melting (very rare)
- Further progression (uncommon) - some patients may require repeat CXL if the first treatment is unable to fully stop the progression (this is more common in younger patients).

© Copyright. All rights reserved.
We need your consent to load the translations
We use a third-party service to translate the website content that may collect data about your activity. Please review the details in the privacy policy and accept the service to view the translations.